Former Pro-Chancellor and Chairman of Council, Federal University, Lokoja, Nigeria. February 2016.
Member, Court of Governors, College of Medicine, University of Lagos, October 2015 for four years.
If you ask me why there is a Medical Women Association without a corresponding one for men, my answer would be that women are a special breed. For how else can one explain all that women are able to achieve as mothers, care providers, teachers, home builders, nation builders and growers of the economy despite the overt and covert discriminations that they suffer.
Women carry the burden of two thirds of the total hours of the work performed. For this they earn 10% of the world’s income and own but 1% of the property. Regarded, paradoxically, as the bedrock of societies, women produce more than one half of the locally grown food in developing countries and as much as 80% in Africa. Activities like food preparation and cooking are almost exclusively the responsibility of women; yet in many cultures, they are often the last in the family to eat, and they take less than other family members (1, 2, and 3). By breastfeeding and caring for the newborn, women provide Primary Health Care and Basic Education of immeasurable dimension and in most instances, their concern for the wellbeing, safety and progress of others far outweighs theirs for themselves.
It is this anxiety for the wellbeing of others that has enabled Medical Women in Nigeria to identify another level of conscientiousness for themselves, “where they as women physicians can make unique contributions to their communities” under the aegis of the Medical Women Association of Nigeria (MWAN) and within the parent body of the Nigerian Medical Association (NMA). I congratulate you, not just on the inauguration of your Association in 1977, but also on your ability to have kept it alive and thriving for so long. May I also take this opportunity to congratulate Drs. Eleanor Nwadinobi and Claribel Abam; Dr. Nwadinobi, your immediate past President on her recent appointment as the sub-Saharan Regional Chairperson for Non-Governmental Organizations (NGOs) by the United Nations Organization and Dr. Abam for taking up the mantle of leadership as the President of this great Association in two days time.
Emerging Diseases
The theme of your conference this year, the 13th in the series, is Emerging Diseases which are described as
diseases that have newly appeared in a population
or those that have existed in the past, but are rapidly
increasing in incidence or geographic range(4).
Medical literature lists a number of diseases, particularly of infectious nature, as belonging to this group. Only a few of this large number are probably of some relevance to our circumstances and of these, the Viral Hemorrhagic Fevers to which group diseases like Lassa fever, Dengue and Ebola belong, will probably come first. In addition, the clostridium virus that causes botulism, variola that causes smallpox, salmonella that causes salmonellosis, H5N1 avian flu virus that causes avian influenza or bird flu disease and the SARS virus that causes Severe Acute Respiratory Syndrome, are also important to us. I do not intend to dwell on these acute infections as I am sure other speakers would do justice to them except perhaps to say that bearing in mind the ferocity with which some of these infections spread and cause disabilities and fatalities once they are allowed to establish a foothold,
the Public Health Measures that are required for their control:
Awareness, Notification, Isolation, Contact Tracing, Quarantine,
Culling of Hosts or Vectors, Vaccination, Vigorous Treatment of
Affected Persons are all measures with which every doctor
should seek to be familiar.
MY TEXT
For my text, I will rather select some diseases which derive partly from your sub-theme and which still fit the bill of Emerging Diseases, especially when widely interpreted, and address them in a concise manner. In the process, I will draw attention to the continuing challenges in the fight against these diseases and how a Change in Life Style could serve as preventive measure or a shield to ameliorate the ill effects of some of these conditions.
HIV/AIDS which is now practically a sub-Saharan African problem, is not only relatively new, it is also currently wearing a “woman face”. Tuberculosis (TB) has become a re-emerging problem, propelled by raving poverty, deprivation and the advent of AIDS, while Malaria, despite efforts at Roll Back Malaria (RBM), has continued to decimate pregnant women and new born babies as well as displaced persons from conflict affected zones and international travelers from malaria free zones of the world. Above all, worldwide, 15,000 people die of AIDS, TB and Malaria everyday; women, along with children, being among the most vulnerable groups to all three diseases in Africa. It comes as no surprise therefore that these three diseases currently engage the attention of the International community in a remarkable manner and combating them was accepted as Millennium Development Goal (MDG) by 189 Heads of State in September 2000.
HIV AIDS / TUBERCULOSIS / MALARIA
HIV/AIDS
The World Health Organization (WHO) defines a pandemic as
an outbreak of an infectious disease that spreads easily
and in a sustainable manner among humans, across a
large region, or even the world.
Of this, history is replete with pandemics that almost annihilated large sections of the human race on several occasions. But no one would have forecast the speed of spread, level of desolation and extent of destruction which the Human Immunodeficiency Virus (HIV) and the Acquired Immunodeficiency Syndrome (AIDS) which it causes, have afflicted on mankind. First discovered as a new disease among young homosexual men in New York and Los Angeles, in the United States of America, it was soon confirmed that the condition is caused by a retrovirus which attacks the natural immune system of the body, thereby making it possible for many different infectious diseases, including those called opportunistic infections that are usually only able to strike when the body’s defenses are weakened, to take hold of the affected.
Over time however, HIV has become essentially an African, and in particular, a sub-Saharan African problem where more than a third of those dying from the disease occurs, retarding economic growth and deepening poverty. Africa with just over 10% of the world’s population carries well over 75% of the burden of the disease and in 2005 lost 2.4 million adults and children to AIDS. (7, 8).
Southern Africa is home to 15 million people living with AIDS or 40% of the world wide total of 40 million people living with the virus. In Zimbabwe, at least 3,000 people die each week from AIDS related illnesses in the country of some 12 million people and early this year, South Africa, where 1,500 new infections and about 900 deaths occur each day, mounted a new and more vigorous 5-year response against the infection under the direct supervision of the country’s Vice President, castigating itself that it had not done enough to change peoples’ sexual behaviour.
Rather unfortunately, women, including married women, increasingly have to bear a greater portion of the burden of the disease especially in sub-Saharan Africa where almost 57% of all individuals living with HIV/AIDS are women (9). For Africans ages 15-24 living with HIV/AIDS, women account for 76% of all infections. In South Africa, Zambia and Zimbabwe, young women ages 15-24 have rates of infection that are between three and six times that of their male peers; while in Nigeria, the National Reproductive Health Survey of 2003 showed that young girls have a twice higher risk of contracting the HIV than boys of their age.
Nigeria’s first two AIDS cases were diagnosed in Lagos in 1985 (10). The country immediately mounted an AIDS programme and appointed a medical woman (like you) to head it. She left a couple of years thereafter when support for the programme had all but disappeared (11). Thereafter, a renewed effort was made to strengthen the response to the epidemic; the Presidential Council on AIDS and the National Action Committee on AIDS (NACA) were established in 2000. These bodies have facilitated a coordinated multisectoral response through the provision of comprehensive prevention and care services within the context of the HIV/AIDS Emergency Action Plan (HEAP), Health Sector Plan and National Strategic Framework (NSF) (12).
A biennial HIV sentinel survey which was started in 1991 aims at determining the HIV prevalence among pregnant women attending antenatal clinics, assessing the trend in HIV prevalence and also providing data for the projection of the epidemic in the general population. The results of the latest survey, that of 2005, gives information on our current knowledge of the epidemiology of the disease in Nigeria.
Overall, the prevalence rate was 4.4%, having declined from peaks of 5.8% and 5.0% respectively in 2001and 2003. Some parts of the country are worse than others, Benue State has a prevalence of 10.0%, Rivers, 5.4%, while Oyo has one of 1.8%, but no State or community in the country is unaffected (Figs. and II).
With these prevalence rates, the infection has extended beyond high risk groups and can rise exponentially. The infection is still more prevalent in the 20-29 year age group and also in Female Sex Workers whose prevalence rate has soared from 17.5% in 1991, through 22.5% in 1993, to a current 35.6% in 2005. Female Sex Workers, therefore, constitute an important reservoir of HIV infection for transmission to the general public through sexual networking (12). Furthermore, the level of HIV prevalence among pregnant women attending antenatal clinics calls for concerted measures to tackle mother to child transmissions.
In March 2007, the Director General of NACA, which has now been transformed into the National Agency for the Control of AIDS, hosted a World Press Conference in Abuja and gave a number of vital information on the disease: about 3-3.5 million Nigerians now live with the virus, and of these, only 100,000 are receiving Anti retroviral treatment (ART) at selected tertiary health institutions. The next phase of expansion of ART would be established in secondary health institutions across the country. Funding for the control of AIDS increased from N300,000.00 in 1998 to about N7.6 Billion in 2006. Access to ART for infected persons and the prevention of fresh infections, therefore, constitute some of the main challenges facing HIV control in Nigeria. In Rivers State, 4,417 are enrolled for ART mainly at the University of Teaching Hospital and the Braithwaite Memmorial Specialist Hospital, also in Port Harcourt.
TUBERCULOSIS
Again, Africa accounts for more than a quarter of all the TB cases in the world and the epidemic continues to increase in Africa despite the implementation of effective TB control strategies. Approximately 35% of all TB patients in Africa are HIV-positive and in 2003, an estimated 80% of the people co-infected with TB and HIV who died, were in Africa. HIV is the main reason for failure to meet TB control targets, particularly in sub-Saharan Africa. This synergy between the two infections, which has necessitated the slogan, One Patient, Two Diseases, constitutes a major challenge in the efforts that are aimed at their control.
Nigeria is one of the 22 countries of the world with the highest burden of the disease where it ranks 4th and 1st in Africa. The incidence in the country is reported as 293 cases per 100,000 per year (13) and 25-45% patients with HIV presenting for ART access have TB.
MALARIA
There is no shortage of words or statistical data in the literature to confirm that malaria accounts for a disproportionate share of ill health and deaths among many nations of the world, especially those in Africa and with particular reference to those in sub-Saharan Africa where the disease also presents major obstacles to social and economic development.
There are at least 300 million acute cases of malaria each year globally, resulting in more than a million deaths. Around 90% of these deaths occur in Africa, where a child dies every 30 seconds commonly from P. Falciparum, the most dangerous form of the infection. Malaria is Africa’s leading cause of under-five mortality (20%) and constitutes 10% of the continent’s overall disease burden. It accounts for 40% of public health expenditure which amounts to about US$ 12 Billion every year, 30-50% of inpatient admissions, and up to 50% of outpatient visits in areas with high malaria transmission. Malaria and poverty interact in a vicious circle and recent evidence suggests that there may be a link between malaria and HIV: malaria infection during pregnancy may increase the risk of mother-to-child transmission of HIV. Indeed, in many ways, Africa’s future development is inextricably linked to the success of malaria and HIV/AIDS prevention and control.
Malaria remains a major public health challenge in Nigeria, with high and escalating infection rates. These increasing infection rates have been made worse by the deteriorating environment which enhances vector propagation and the appearance of strains of the infection which are resistant to cheap chloroquin and thus require more expensive artemisinine containing compounds for their control (13)
So intense has been the local and International response to the control and eradication of these three infections globally but especially in Africa, in accordance with the demands of MDG 6, that it will be outside the scope of this paper to discuss them in any detail. Just a mention of a few of them and some possible outcomes will suffice. They include PEPFAR, Bill Clinton Foundation, Belinda and Bill Gates Fund, Roll Back Malaria.
However, the point must be made that the preference for the adoption, by donor agencies, of these “vertical programmes” as they are known, as opposed to the strengthening of the overall health systems of poor countries through support for the provision of universal access to basic health care is being criticized as not being in the best interest of the affected countries. .
UNSAFE ABORTION / MATERNAL MORTALITY
In Nigeria, where the practice of abortion is restricted by the legal instruments of the Penal and Criminal Codes, out of about 7 million pregnancies that occur each year, about 11% end up as induced abortions, indicating that not less than 610,000 procured abortions are performed each year, at a rate of about 25 abortions per 1000 women aged 15-44 years (15). Of these, adolescents between 15 and 24, the same target group as is for the HIV/AIDS pandemic, are in preponderance.
The majority of these abortions are carried out by physicians and other trained health workers in clinics and hospitals and are often free from complications. Still, unsafe methods continue to be widely used, especially by non-medically trained workers, resulting in severe health consequences for about one in four women who terminate their pregnancies (16, 17).
Unsafe abortions contribute to the nation’s high maternal mortality rate in a variety of ways, including trauma to vital organs, haemorrhage, septicaemia, renal and hepatic failure. For those who do not die, recurrent pelvic infections giving rise to persistent ill health and secondary infertility from chronic pelvic inflammatory disease, are real dangers to contend with. While in economic terms, unsafe abortions drain the country’s health care infrastructure as medical establishments are obligated to allocate scarce medical resources and personnel to assist women suffering from life-threatening complications.
With regard to the bigger picture of maternal mortality, like the reduction in deaths from AIDS and Malaria, the issue of reduction in the number of women who die as a result of pregnancy and its consequences, is now regarded as a development matter which has to be addressed in order to build a better and more equitable world. This was the position of 189 Heads of State and Governments when they gathered in New York in September 2000 at the Millennium Summit to reflect on the common destiny of mankind and to construct “a blueprint for building a better world in the 21st century”.
The fact that maternal mortality is a development matter as is indeed expressly stated in the 5th MDG is easy to comprehend as 99% of such deaths occur in underdeveloped countries. Furthermore, the number of maternal deaths worldwide per 100,000 births is 430, with a sharp division between developing countries, where the maternal mortality ratio is estimated to be 480, and developed countries, where the ratio is 27. These ratios can be translated into women’s lifetime risks of dying from pregnancy/pregnancy-related reasons: 1 chance in 48 in the third world contrasted with 1 in 1,800 in developed countries. The highest maternal mortality levels are found in parts of India, eastern and western Africa with some of the least developed countries of the world (800-1,000 per 100,000 births in Nigeria); the lowest levels occur in northern Europe with some of the best developed countries of the world (<4 per 100,000 births in Finland).
Nigeria, situated on the West coast of Africa, has some of the worse statistics relating to maternal mortality in the developing world. Worldwide, an estimated 529,000 women die each year from the complications of pregnancy and childbirth, essentially from 13 underdeveloped countries. Of these, 55,000 deaths occur in Nigeria alone. Thus, although Nigeria accounts for only 2% of the world’s population, it produces 10% of the global estimates of maternal deaths. The only country that has a higher absolute number of maternal deaths is India with 136,000 maternal deaths each year (18, 19, and 20).
More than 70% of all maternal deaths in Nigeria are due to five major complications of pregnancies: circulatory collapse from ante and/or post partum blood loss, severe genital tract infections during or after parturition leading to septicaemia, obstructed labour and its sequelae, hypertensive disorders of pregnancy, and complications of unsafe abortion. In most instances the conditions that cause death are preventable and treatable but mothers still die on account of a number of factors: widespread poverty resulting in inability of some to access or pay for medical services; ignorance which precludes those affected from utilizing existing medical services and weak health infrastructure with a very poor referral system which is unable to respond satisfactorily and swiftly to the demands of critically ill patients.
Again for maternal deaths, since the ground-breaking Safe Motherhood Conference of 1987 in Nairobi, Kenya, global attention has been directed to the issue as has never been the case before. At the country level, only last year, the former President, Chief Olusegun Obasanjo, appointed a Special Adviser on Maternal Health, and followed this up with the announcement this year, that medical care for all pregnant women and children under five, are now to be free in all Federal Government-owned Health Institutions, a measure that was already in place in some States in the Federation, including Rivers State, the venue of your 2007 conference. Furthermore, the wife of the current President, Ahjia Turai Yar’ Adua, has made it known that she would mount programmes that will aim at reducing maternal and childhood mortalities. These measures, coupled with the on-going reactivation of Primary Health Care (PHC) centres across the country, the revamping of tertiary hospitals via the VAMED programme, and the proposed inclusion of Midwifes into the National Youth Service Corps (NYSC) programme, are seen by many as bold steps which ultimately should help in reducing the number of women who die in pregnancy-related circumstances.
BREAST CANCER / CERVICAL CANCER.
Patients with breast cancers in African populations tend to be young (average age 44 years) with about 86% of them presenting with large advanced tumours – a situation which most times allows hygienic mastectomy as the only means of intervention. This contrasts with the situation in the Caucasians where the disease is commoner in obese postmenopausal women (average age 55 years) and with less extensive growths – permitting the use of a wider array of curative measures. Accordingly, the five year survival rate of 85% in the Caucasians is markedly different from that in Africans, which is a mere 10%.
Self breast examination which should be taught at schools remains an important way of identifying early cases of breast cancer. Also child bearing is known to protect against the disease and so does breastfeeding. On the whole, the longer a woman breastfeeds, the more she is protected against breast and ovarian cancers.
Over 80% of mortalities from carcinoma of the cervix occur in developing countries, usually from advanced end-stage disease. In Nigeria, the disease is found in parous women in their 40s and 50s and because presentation is usually late, treatment options are very limited.
Apart from healthy living, expanded national cervical cytology screening through pap smears seems to be the way by which developed countries have brought down deaths from cervical cancers. It is therefore unfortunate that in many developing countries, there are no national cancer screening services. Efforts by the Rivers State branch of your Association and that of the current wife of the Bayelsa State Governor in establishing screening centres for these cancers must be commended.
The risk factors for the disease include early coitus, tobacco, sexually transmitted disease especially Chlamydia, Herpes and types 16 and 18 Human Papilloma Virus (HPV) infection. HPV, a group of DNA viruses, which are common infections especially in the US are recently attracting a lot of attention. Although infected individuals may be symptom free, infection with HPV has been associated with the formation of vaginal and anal warts, vaginal cancer, cervical dysplasia, cervical cancer, and colon cancer. It is for these reasons that a new vaccine, Gardasil Vaccine, is being developed to fight the infection.
As prevention against carcinoma of the cervix, it is planned to vaccinate young girls between the ages of 9 and 26 years in three separate injections over a period of six months (0,3,6), before they commence sexual intercourse with Merck’s quadrivalent HPV vaccine, Gardasil, which has now been licensed in more than 45 countries.
OBESITY / DIABETES MELLITUS / HYPERTENSION
These non-communicable diseases which are now called by many names – diseases of affluence, silent killers, stealthy killers, on account of their insidious nature, are creeping up to becoming serious problems everywhere, including Africa. They are closely related as obesity not only triggers Diabetes and Hypertension, it also makes their control that much difficult. Taken together, they constitute the commonest cause of sudden death in any society and their prevalence is on the increase in African communities due to ageing of the population and drastic lifestyle changes accompanying urbanization and westernization (23). They are associated with long term chronic debilitating conditions, especially atherosclerosis – a build up and hardening of fatty deposits within blood vessels, resulting ultimately in blockages. Left unchecked therefore, they will apply serious pressures on health delivery systems in the future particularly in African countries. Furthermore, one single organ – the Heart- seems to bear the brunt of all three diseases more than others- information to which many are complacent. As the saying goes, You have only one heart – treat it with extra care .
Obesity has been described as an epidemic out of control as over 350 million people globally are obese (Body Mass Index of 30 and above) and about 1 billion, overweight ( BMI of between 25 and 30). In the US, 30% of adults are obese and 65% overweight. Levels are similar in South Africa, where, paradoxically, as many as are obese also die from malnutrition. Obesity is also common in Nigeria especially in market women. (BMI=wt in kg divided by height in metres square. Wt.Kg/Ht.m2 ).
Being overweight and obese is associated with a higher risk of disease particularly if body fat is concentrated around the abdomen. The disease outcomes for the overweight and obese include Type 2 Diabetes, Ischaemic Heart Disease, Stroke, Hypertensive Disorders, Osteoarthritis, Cancers (colon, kidney, endometrial, post menopausal breast cancer).
In contrast to the writing of a British doctor on the diseases he met in Africa that diabetes is very uncommon but very fatal in 1901 (24), there is now a global trend towards an increase in the incidence and prevalence of Diabetes Mellitus in African populations (25) which was estimated at 3 million in 1994 and is expected to go through a 2-3 fold increase by the year 2010 (26). This increase in prevalence is due to energy intake which now exceeds expenditure resulting in large number of individuals with more body fat relative to muscle mass (Fig.3).
Outside age and ethnicity as risk factors for the disease, urbanization, with its characteristic Lifestyle, seems to have played a major role in the rapid increase in prevalence of the disease as urban residents have a 1.5 to 4 fold higher prevalence of diabetes compared to their rural counterparts (27). In many African cities, urban life is characterized by changes in dietary habits involving an increase in the consumption of processed food items like refined sugars and saturated fat, and a reduction in fibre intake (28). Furthermore, whereas rural populations rely on foot walk as transportation means and often have intense agricultural activities as their main occupation, reduction in physical activity is associated with urban living (29).
Hypertension, a completely treatable condition, defined as a blood pressure reading of 140/90mmHg and beyond, is the most common cardiovascular condition in the world. It completes the triad of the dangerous non-communicable diseases that are now posing important threats to the health of many adult Africans. Cohort studies on hypertension in Nigeria and Zimbabwe and epidemiological information show that between 10 and 20 million people in sub-Saharan Africa may have hypertension and that treatment could prevent around 250,000 deaths each year.
In Africa, as elsewhere, obesity and sodium intake are major risk factors for hypertension (31) and mortality from the disease, mainly from stroke and congestive heart failure, may vary from 5-15% (32). Human beings ordinarily consume more sodium than potassium and suffer average rise in blood pressures with increasing age and so, not infrequently, become hypertensive as they advance in age. It is in the light of this fact that investment in an organized care system for the prevention as well as for the sufferers of this disease has been advanced as one that would reap large gains in adult health (33) (Fig.4).
VIOLENCE AGAINST WOMEN
In Nigeria, as is elsewhere, gender-based violence as it affects women is manifested in many forms, including physical violence, sexual abuse, genital mutilation, trafficking of women and girls and child marriage – time will allow only a cursory elaboration on just a few of these.
The term “trafficking in persons” is restricted to instances where people are deceived, threatened, or coerced into situations of exploitation, including prostitution. Trafficking of Nigerian girls and women, usually between the ages of 17-20, to Europe for prostitution, which began in 1992, has become a big business in recent times. The largest group of prostitutes in Western Europe from sub-Saharan Africa comes from Nigeria while Italy remains the country of first choice for would-be Nigerian prostitutes probably because prostitution is legalized in that country.
Trafficking from Nigeria is especially well organized and centers around a female figure called “mama” who plays a key role in deceiving young women to leave their homes for Italy where they function as street prostitutes, constituting the low-wage earners in the prostitution market with their places of work (joints) often located in the suburbs or along major highways. Once trafficked to Italy, very few show willingness to return to Nigeria, citing lack of opportunities, fear of reprisals from traffickers, and the shame of returning without visible evidence of success in financial terms.
Female Genital Mutilation (FGM) or Female Genital Cutting (FGC), also known as Female Circumcision (FC), is a practice that is widespread in Nigeria, embraced to varying degrees, as a cultural dictate, by many ethnic groups in the country. Estimates obtained from the 1999 Demographic and Health Survey indicated that about 25.1% of women had had one form or the other of this surgical operation.
Referring to this unfortunate act, the then President of your Association, Professor (Mrs.) Oyin Elebute, in her Opening Address at your third biennial conference in Enugu, on 7 May 1983, described it as the “unkindest cut of all”, burrowing from a publication in the London Sunday Observer of April 16, 1979.
The erroneous belief is that uncircumcised women are promiscuous, unclean, unmarriageable, physically undesirable and /or potential health risks to themselves and their children, especially during childbirth. One traditional belief is that if a male child’s head touches the clitoris during childbirth, the child will die (34).
Of the four known types – types I (removal of the hood of the clitoris) and II (excision of the clitoris) are the most frequently practised in the country. Practise of the more dangerous types III (excision of all parts of the external genitalia) and IV (introduction of corrosives into the vagina), are, fortunately, uncommon (Figs. 5 and 6).
While it is doubtful if any good follows any type of female circumcision, the condition, especially in the cases of types III and IV, is clearly associated with social as well as medical complications which could be life threatening especially during labour. Aside from compromising the pleasure which sexual stimulation of the clitoris brings about, FGM can lead to infection, haemorrhage, vaginal stenosis, infertility and obstructed labour.
Happily, the practice is currently receiving widespread condemnation in the country from NGOs, Cultural organizations, Professional Bodies, Women’s Organizations and various Governments which are even instituting legislations to make the practice actionable as a criminal offence.
CHANGE IN LIFE STYLE AS ANTIDOTE
Not all the diseases we have discussed lend themselves to cure or even amelioration through Changes in the Way We Live. For some, individuals will require support and actions by communities, health institutions and governments for prevention and cure. For example providing decent living accommodations for people with rooms that are well-spaced and ventilated is an important public health measure to combat tuberculosis as such environments avoid overcrowding. Also mention has been made of some of the actions which Government is taking that are expected to cut down on the number of women who die in pregnancies and related conditions.
But in the cases of a number of the diseases there exit ways by which individuals can improve their chances of survival by Changes In Their Life Styles. It is to these measures that we must now direct our attention during the remaining minutes of this lecture and indicate Patterns of Life Style that Promote Healthy Living. Although the emphasis is on an overall promotion of health, we shall, as much as possible, relate the patterns to some of the diseases we have discussed.
Although HIV can be transmitted through the transfusion of infected blood as well as the sharing of infected needles, the major means of acquiring the infection is through unprotected bi or homo sexual intercourse with an infected partner. Whereas the danger of infection is practically non-existent in a mutually faithful relationship, sexual intercourse practised in multiple relationships, casually or with prostitutes, through the oral, vaginal or anal routes, constitutes important portals of transmission of the virus. This is more so in the instances in which the condom is not used for protection during such Risky Sexual Behaviours.
Sexual intercourse also in the circumstances that have already been described, is a significant way of passing on other Sexually Transmissible Infections (STIs), notably, HPV – associated with cervical cancer, Chlamydia – associated with infertility, and Gonorrhoea – also associated with infertility.
Furthermore, early sexual activities constitute risk factors for cervical cancer and sexual intercourse is a forerunner to an unwanted pregnancy which could end up as an unsafe abortion.
In general, smoking reduces the health of smokers by harming nearly every organ of the body and causing diseases. More deaths are caused each year from tobacco use than by all deaths from HIV infection, illegal drug use, alcohol use, motor vehicle injuries, suicides and murders combined (35). Tobacco is related to cancers including cancers of the lungs, bladder, oral cavity, cervix, kidneys, and stomach. It also causes coronary heart disease, stroke, vaso – constriction, chronic obstructive lung diseases and bone demineralization in post menopausal women.
Although available information indicates that cigarette smoking in Nigerian females is relatively low (36), the long list of diseases caused by smoking should ensure that the practice is not encouraged at all. Of course, it goes without saying that other forms of drug abuse which are imbibed through smoking, like marijuana, should be completely tabooed.
Overwhelming evidence now exists to show that moderate regular alcohol consumption (men, 3-4 units; women, 2-3 units per day. 1 unit = 10ml pure alcohol) is good for health. Moderate drinkers tend to have a better life and live longer than total abstainers or heavy drinkers. In addition to having fewer heart attacks and strokes, moderate consumers of alcoholic beverages (beer, wine or distilled spirits or liquor) are generally less likely to suffer hypertension, peripheral artery disease, Alzheimer’s disease and the common cold. Sensible drinking also appears to be beneficial in reducing or preventing diabetes mellitus as well as a number of other conditions. In sum, moderate consumption of alcohol appears to be more effective than most other life style changes that are used to lower the risk of heart and other diseases as it increases HDL (“good”) cholesterol, decreases LDL ( “bad”) cholesterol, reduces platelet aggregation, increases fibrinolysis, and increases coronary blood flow (37).
However, these health promoting properties of moderate alcohol intake must be juxtaposed against the ill effects of heavy consumption resulting in alcohol abuse- a pattern of drinking that results in harm to one’s health, interpersonal relationship or ability to work. The important thing is to know where the benefit ends and the risk begins.
Furthermore, alcohol should be completely avoided in pregnancy because of the risk of fetal Alcohol Syndrome which is the most severe form of the Fetal Alcohol Spectrum Disease (FASD).
Exercise is good for the body. From preventing heart disease and type 2 diabetes to managing weight and stress, to maintaining fitness, regular physical activity helps extend life and improves its quality. Like moderate alcohol intake, exercise lowers the build up of plaques in arteries by increasing the concentration of high density lipoprotein cholesterol while lowering that of low density lipoprotein cholesterol. Exercise also increases heartbeat and pumps more blood round the body. This increased pumping helps to dislodge plagues that may be forming on the walls of the vessels and so reduces the chances of developing heart attack.
In addition exercise lifts frail spirits, fights depression and reduces the risk of certain types of cancers like colorectal and breast cancers.
Moderate intensity physical exercise which involves the burning up of 200 calories per day – equivalent of brisk walking of 30 minutes every day is enough to bring about real benefits in terms of preventing illness. Other forms of exercises involve cycling, swimming and jogging. The best exercise to change our sedentary habits is the one we can and will do nearly everyday.
Eating healthily and properly reduces the risk of diseases and is effective against weight gain. Meals consisting mainly of grains, fruits and vegetables with reduced amount of meat, cheese and butter are recommended. Consumption of fish, fish oil and foods high in potassium (e.g. sweet potatoes, plantains, bananas, fruit juices) is also associated with reduced risk of cardiovascular diseases (38).
Fruits and vegetables contain essential minerals and vitamins that are needed for the proper functioning of the body and for protection against diseases. Carotenes present in green leafy vegetables and coloured fruits and vegetables act as antioxidants which guide against heart disease and cancers by interfering with the damage caused by free radicals which include superoxides or Reactive Oxygen Species (ROS) (38). Antioxidants, such as beta-carotene, vitamins A, C and E, also retard the aging process, avoid memory loss and are effective against constipation. Furthermore, fruits and vegetables contain salicylic acid and this explains the low levels of heart disease among those who eat a lot of fruits and vegetables.
Most of the chronic non-communicable diseases of modern man arose because of departure from the diet of our ancestors. Therefore, to reverse the trend of rising incidence of chronic non-communicable disease, man must return to the diet to which his genes have been accustomed for over 2 million years (38).
On the whole, being overweight is associated with a poorer functional status – pain, worry, restricted activity and undisputed adverse consequences for health, especially cardiovascular diseases, glucose intolerance and malignant disorders. Additionally, there is evidence to show that overweight and obesity increase the risk of cancer of the breast and many others. Dietary factors are only second to tobacco as avoidable causes of cancer (38).
Decrease in calorie intake by eating less and increase in physical activities are recommended ways for weight reduction. However, it must be realized that reducing and piling up weight again may also have adverse health consequences. Maintaining a healthy weight is not just about going on a diet and coming off a diet when one reaches a target weight. It is adopting skills that change one’s eating habit for life.
Efforts should be made to combat the stress of daily living, which reduces productivity, depresses the immune system and generally renders the body to be more prone to ill health, by engaging in various forms of relaxations – recreational sports, watching movies, taking internal and external holidays. Furthermore, it helps to have a positive attitude to life and a hobby outside one’s main profession, in addition to being creative, innovative and happy. Adherence to a religious belief which is practised faithfully results in internal peace and is an effective antidote to stress and the vicissitudes of earthly existence.
Regular medical examinations, even in the seeming absence of ill health during which history is taken, clinical examination carried out and some laboratory investigations done is an important measure for assuring good health which is not taken seriously enough by many, including doctors themselves. Such examinations should be carried out at least once a year but more frequently in the elderly. Their value lies in their preemptive nature by which several diseases whose onsets are slow – hypertension, diabetes, some cancers, can be detected early and appropriate management instituted with better overall prognosis. It is this fact that has now brought about the establishment of Well People’s Clinics in some parts of the industrialized world.
CONCLUSION
Abimbola Awoliyi, nee Akerele, was not only the first Nigerian female Obstetrician and Gynaecologist, she was also the nation’s first female medical doctor. Of her, indeed it can truly be said that she lived up to the tenets of her profession – that of offering to all women, within and outside of pregnancy, the highest possible level of care that would enable them attain a state of physical and mental wellbeing.
Commencing her professional career at the General Hospital, Lagos, the country’s oldest hospital, after her medical training in the Republic of Ireland, , she subsequently worked in various parts of the country, including Aba, in present day Abia State and there, as well as in others, endeared herself to the poor and lowly. She returned to Lagos and was eventually given charge of the Island Maternity Hospital, Lagos, a bustling baby factory even in those days. Little wonder that there is now a Hospital and a road named after her in the city of Lagos as worthy and earned reminders of her legacy.
The over-arching characteristics of her life were doggedness, determination and intense personal discipline which are also the hallmarks of those with Life Styles that ward off or ameliorate some of the diseases we have discussed. The abstinence, commitment to mutual faithfulness and condom use in sexual relationships which serve as insurance templates against contracting HIV, require determined and disciplined pairs. So also is the refusal to engage in a Risky Sexual Behaviour that could lead to an unwanted pregnancy and an unsafe abortion.
As for the avoidance of smoking, engagement in regular physical exercises, moderation in alcohol intake, maintenance of appropriate weight, and healthy eating – the bedrocks of heart health, only successful adherents can attest to the level of personal commitment, resolve and tenacity, just like what Abimbola Awoliyi exhibited in her personal life and professional career, that is required to institutionalize them as a way of life.
An Officer of the Federal Republic of Nigeria (OFR) and also of the British Empire (OBE), Abimbola Awoliyi was a roundly developed woman including in her relationship with her Creator, “where her spiritual development appeared to have increased rather than embittered by tragic circumstances. One of these tragic occurrences happened in Aba. Her child contracted measles after playing with other children who also had measles. She toiled hard to save these children. They survived but hers died of respiratory complications” (39). Again, it does not come as a surprise therefore that she was the first female Nigerian to be honoured by the Pope.
With a high burden of disease in Africa, including Nigeria, characterized by a wide array of infectious disorders, trauma and non-communicable ailments, which exist against a backdrop of poor and inadequate health services as well as constraints to socio-economic development, individual Nigerians must learn to assume some responsibilities for the maintenance of their own health by taking proactive actions on best practices that support good health – a factor that is now emerging as one of the basis to hire and fire in some countries. Abimbola Awoliyi, in her life time supported those public health measures that emphasized prevention as antidote to curative hospital care.
Today’s lecture advocates for no less and challenges all medical women to not only “Heal with the Spirit of a Mother (Matris Animo Curant)”, the motto of your Association, but also to be in the vanguard of educating Nigerians, rural as well as urban dwellers, on those Life Styles that are Salutary to Health.
FIG 1
HIV Prevalence Sentinel in Nigeria
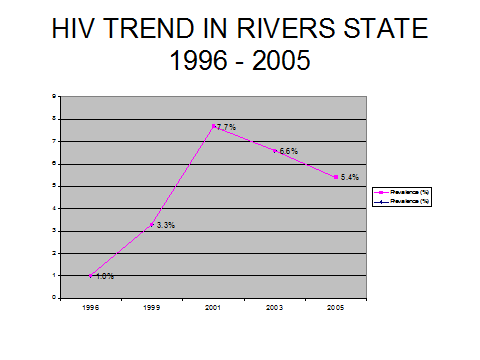
FIG 4
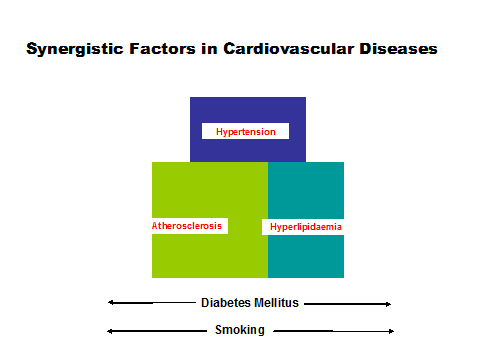
FIG 2
Fig 4
Fig. 5
TYPE II FGM
Fig. 6
REFERENCES
13 MDG5: What Path leads to its Achievement in Nigeria? A Guest Lecture by Nimi D. Briggs
On the occasion of the 7th International Conference of the Society of Gynaecology and
Obstetrics of Nigeria (SOGON). Wednesday 22 November, 2006.
14The Global Plan to stop TB 2006-2015-Actions for Life-Towards World Free Tuberculosis. WHO, 2006.
15Henshaw Sk; Singh S; Oye-Adeniran B; Adowole IF et al (1998).The Incidence of Induced Abortions in Nigeria. International Family Planning Perspective; 24, 156- 163.
16Archibong EI; (1991).Illegal Induced Abortion-a continuing problem in Nigeria. International Journal of Gynecology and Obstetrics; 34(3): 261-265.
17Ladipo AO; Illegal Abortion and effect on medical practice and public health-Nigeria, in Landy U and Ratnam SS, eds..,Prevention and Treatment of Contraceptive Failure, New York: Plenum, 1986: pp. 53-60.
18 Nigeria Health Review 2006. Health Reform Foundation of Nigeria (HERFON).
19World Health Organization. Life Time Risks of Maternal Deaths. Geneva: WHO, 2004.
20National Planning Commission. Children and Women’s Rights in Nigeria: A wake-up Call. Situation Assessment and Analysis 2001.
21Lev-Ran A (2001) Human obesity: An evolutionary approach to understanding our bulging waistline. Diabetes Metab Res Rev 17: 347-362.
22 Stoll BA; Upper Abdominal Obesity, Insulin resistance and breast cancer risk. Int. J. Obs Relat Metab Discord 2002;26: 744-753.
23Gwatkin D, Guillot M, Heuveline P. (1999).The Burden of Disease among the global poor. Lancet, 354, 586-589.
24Cook AR. (1901) Notes on the diseases met with in Uganda, central Africa. J Trop Med 4, 175-178.
25King H, Aubert RE, Herman WH. (1998) Global burden of diabetes. 1995-2025: prevalence, numerical estimates and projections. Diabetes Care, 21, 1414-1431.
26Amos AF, McCarty DJ, Zimmet P. ( 1997) The rising global burden of diabetes and its complications:estimates and projections to the year2010. Diabet Med. 14,81-85
27Gill G, Mbanya JC, Alberti KG, Diabetes in Africa 1997, Cambridge
28Sharma S, Cade J, Jackson M et al. (1996) Development of food frequency questionnaires in three population samples of African origin from Cameroon, Jamaica and Caribbean migrants to the UK.Eur. J Clin Nutr 50, 479-486.
29Alemu T and Lindtjorn B. Physical activity, (1995) illness and nutritional status among adults in a rural Ethiopian community.Int J Epidemol, 24, 977-983.
30Sobngwi E, Mauvais-Jarvis, Vexiau P, Mbanya JC,and Gautier JF (2001) Diabetes in Africans. Review. Diabetes Metab 27,628-634
31In: Akinkugbe OO, ed. (1997) Non-communicable diseases in Nigeria:final Report of a national survey. Lagos: Federal Ministry of Health and Social Sciences.
32Azuzu MC, Johnson OO, Owoaje EE,Rotimi CN et al (1996) Questions on adult mortality. World Health Forum 17: 373-376 [ Medline].
33Cooper RS, Rotimi CN, Kaufman J, Muna WFT, Mensah GA (1998).Hypertension treatment and Control in Sub-Saharan Africa: the epidemiological basis for policy. BMJ 316: 614-617.
34Nigeria: Report on Female Genital Mutilation (FGM) or Female Genital Cutting (FGC). U.S. Department of State. Report released on June 1, 2001.
35McGinnis J, Foege WH (1993) Actual Causes of Death in the United States. Journal of American Medical Association 270: 2207- 2212.
36Ibeh CC, Ele PU. (2003) Prevalence of Cigarette smoking in young Nigerian Females. AfrJ Med Sci. 4: 335-8
37Alcohol: Problems and Solutions. Web based information.
38Adelekan, Delana; ( March 13,2007). Diet, nutrition and chronic diseases: What you eat is what you get. Professorial Inaugural Lecture. Obafemi Awolowo University, Ile Ife.
39Belo-Osagie,T; First Abimbola Awoliyi Memorial Lecture. Saturday, 9th May, 1983.
Change in Lifestyle As Antidote to Emerging Diseases, a lecture delivered by Professor Nimi Briggs FAS, University of Port Harcourt, on 20th September, 2007 at the 13th Abimbola Awoliyi Guest Lecture at the 2007 Biennal Conference of the Medical Women Association of Nigeria
Former Pro-Chancellor and Chairman of Council, Federal University, Lokoja, Nigeria. February 2016.
Member, Court of Governors, College of Medicine, University of Lagos, October 2015 for four years.
Copyright © 2025 Prof Nimi Briggs. All rights reserved. Designed by Syllable Media Limited +447869717613