Former Pro-Chancellor and Chairman of Council, Federal University, Lokoja, Nigeria. February 2016.
Member, Court of Governors, College of Medicine, University of Lagos, October 2015 for four years.
Introduction — I wish to start by expressing my profound gratitude to the Council of our great society, the Society of Gynaecology and Obstetrics of Nigeria (SOGON), for giving me the opportunity to deliver this Guest Lecture. This is the second occasion in recent times that such a privilege has been extended to me and I thank Council immensely for its generosity.
Severe deprivation, extreme poverty, pregnancy related deaths, children dying before their fifth birthday, and those alive being out-of-school, the scourge of HIV/AIDS, rapid environmental degradation, some of the core challenges and crises that are addressed in the 8 Millennium Development Goals (MDGs), have been with us in Nigeria for a long time.
About 60% of Nigerians live below the poverty line of one US dollar a day (1) and the income per capita in the country amounts to a mere 60 cents per day (2). With a maternal mortality rate of about 800 per 100,000 births, mothers in Nigeria stand some of the highest risks of dying during childbirth (3). The under five mortality rate of 198 per 1,000 births in the country is among the highest in the world (3) as one in five children die before the age of five (2); these deaths being due mostly to malaria and other preventable diseases. Nigeria is one of four countries (others are Pakistan, India and Ethiopia) whose children account for the 23 Million of the world’s 77 million out-of–school children (4). Nigeria’s primary school completion rate at the national level in 2004 was just 12% and only about 30% of the births of children under five years of age were registered. In addition, 32.6% of females had had circumcision (5).
With a population of about 130 million and an HIV sero-prevalence rate of 5.8% in 2001, 5.0% in 2003, and 4.5% in 2005, Nigeria has one of the largest numbers of persons infected with the virus in the world (6). As a result of the nation’s large population and high sero-prevalence rate along with the associated mortality of the disease, about two million children have become AIDS orphans since HIV infection was first reported in Nigeria in 1986 (2).
Land degradation, rapid deforestation, water spoilage, soil and air pollution from gas flaring and oil spills are issues of serious concern in Nigeria (1).
These problems, coupled with ineffective and non-responsive governance have been some of the causes of mass discontent which have erupted into violence from time to time especially in the oil bearing parts of the country. Not surprisingly, the military also cited them as being some of the reasons behind its repeated seizure of power in Nigeria. One military Head of State, in so doing, described the nation’s hospitals as “mere consulting clinics.”
As it is in Nigeria, so it is also in some other countries, especially in the developing countries of sub-Saharan Africa. This region, with continuing food insecurity, a rise in extreme poverty, stunningly high child and maternal mortality, and with large number of people living in slums, has been described as the epicentre of the crises (7).
In sub Saharan Africa, the number of extremely poor persons doubled from 164 million in 1981 to 313 million in 2004 and the average income of those living on less than a dollar per day fell from 64 to 60 cents (8). Of the estimated 600,000 women who die in pregnancy or childbirth every year, 99% of these occur in the developing world (9). The vast majority of persons living with HIV/AIDS in the world are in sub-Saharan Africa (fig.1).
So it was that at the turn of the millennium whereas some states looked forward to further progress, prosperity, and global corporation, many others, caught up in unending circle of poverty, internecine warfares and degraded environment, barely had a future. But in an exceptional show of solidarity, “all the world’s Governments” came together in 2000 to reflect on their common destiny and to construct “a blueprint for building a better world in the 21st century”.
Taking a cue from their observations at the world’s summits of the 1990s, Heads of States identified the world’s main developmental challenges and responded to them at a Summit in September 2000, at the United Nation’s Headquarters in New York. That meeting, the Millennium Summit, which was attended by representatives from 189 Member States, 100 of them by their actual Heads of State, as well as all the world’s leading development institutions, was the largest gathering of world leaders in human history. The eight UN Millennium Development Goals (MDGs) which were enunciated at that Summit constitute a global strategy for making poverty history and for the building of a better and more equitable world. The goals themselves range from halving extreme poverty to halting the spread of HIV/AIDS; from providing universal primary education to ensuring environmental sustainability; from promoting maternal health to combating child mortality. In a way, they are also basic human rights as they declare the rights of each person on earth to health, education, shelter and security (Fig. 2).
Intended to be achieved by 2015, the MDGs are time-bound with each goal having its target(s) which are designed to provide the nations of the world with a number of tangible improvements to aim for, as well as indicator(s) by which success could be measured. Many of the goals are health-based as if to confirm the adage that it is the health of its people that constitutes a nation’s greatest wealth.
Some of the MDGs can be realised if every one plays his part and the nation’s of the world work together. Poor countries have promised to shun corruption, govern better, and invest in their people through health care and education. On their part, rich countries have pledged to lend support through enhanced aid, debt relief and trade liberalization.
The focus of today’s lecture is on MDG5: the Improvement of Maternal Health. And so we shall dwell on this goal as well as its target of reducing maternal mortality ratio by three-quarters by the year 2015. We shall also examine the indicator for success in MDG5, which is the proportion of births that are attended by skilled health personnel. Because Nigeria represents the environment of our discussion, my treatment of the above issues, shall, essentially, be in that context.
Apart from doing the usual wise things which enhance good health in anybody: the abhorrence of smoking, the avoidance of physical inactivity, the intolerance of overweight, the consumption of alcohol in moderation, as well as sensible eating, the paper states that the path to improving maternal health in Nigeria, involves an integrated range of care which should commence from the early childhood of the female child. With specific reference to reduction in maternal mortality ratio and the enhancement of available skilled care at delivery, the paper argues that an important way by which this can be achieved, is to get basic health services, including maternity care, which is rooted within the context of Primary Health Care (PHC), to women in rural communities where they live and work.
Childhood Care
It would be simplistic for one to think that it is possible for a child to wade through childhood without adequate care, malnourished, with repeated and intercurrent infections, crippled with poliomyelitis, and yet be a healthy mother for child bearing at a later age. Such a woman may not have attained her full growth potentials; her immune system may have been compromised and her growth stunted, with resultant pelvic contraction along with all its problems in childbearing. It is such considerations that make proper care of the female child, part of the process of promoting maternal health.
Of the several measures that are known to enhance child survival and promote the health of children, three are particularly relevant to our circumstances in Nigeria. These are nutrition, immunization, and prompt response to febrile and diarrhoeal diseases.
Nutrition
For many reasons, breastfeeding remains the gold standard for childhood nutrition. It is the best and most complete food that is known for the infant. The antibodies it contains reduce the risk of infection and breastfeeding reduces the chances of acquiring infection through unhygienically prepared supplementary feeds. Breast feeding alone, which is known as Exclusive Breast feeding, which means that the infant receives only breast milk, is sufficient to cater for all the nutritional needs of the child within the first six months of his/her existence. It is the realization of this tremendous advantage and potential of breast feeding to contribute to child health and survival that resulted in a massive promotion of breast feeding through the Baby Friendly Hospital Initiative (BFHI). Hospitals and health facilities, so designated, encourage mothers to exclusively breast feed their new born babies. But although over 1000 hospitals and health facilities are now Baby Friendly, and the breast feeding of new-borns is virtually universal in the country, the proportion of Nigerian mothers who sustain breast feeding is low and practices differ widely.
Nutrition continues to be an important factor for the proper development of the child even after he or she has been weaned off breast milk. Protein energy malnutrition by itself or in combination with other illnesses is a significant cause of mortality among Nigerian children. In recent times, this is being tackled by the Federal as well as State Governments in Nigeria through the School Health Programmes at which meals that are appropriate in quantity and quality are supplied to school children.
Immunization
Childhood immunization is one of the most potent strategies against childhood morbidity and mortality as high vaccination coverage is generally associated with low levels of disease in the population. It is this fact that informs the position of the World Health Organization (WHO) in encouraging nations to institute programmes of childhood immunization for use in their respective countries. The Vaccine Preventable Diseases (VPDs) for which provisions are made under the Nigerian National Programme of Immunization (NPI), are tuberculosis, diphtheria, pertusis or whooping cough, tetanus, poliomyelitis, measles, hepatitis B and yellow fever. Although these infections cause severe ill-health and death in large number of children, they are, happily, highly preventable through effective immunization. Children who receive complete immunization through vaccination are usually protected against the corresponding diseases for life.
In the last decade, due to a variety of reasons, the number of children who receive routine immunization in the country has fallen sharply. With a coverage rate for DPT3 of only 25% in 2005 as reported by WHO, the situation in Nigeria compares very poorly with those of its neighbours where coverage rates as high as 88% and 73% were obtained for Benin and Cameroon republics respectively (Fig. 3).
Febrile and Diarrhoeal Diseases
Infection with malaria parasites especially with plasmodium falciparum is by far the most important cause of ill-health, especially those associated with fever, in Nigerian children. The effect of malaria, which is endemic in the country, starts in the mother’s womb where it could cause low birth weight and premature delivery as a result of maternal pyrexia. Anaemia, haemolytic as well as megaloblastic, which could be so profound as to necessitate red blood cell replacement, constitutes an important complication in children which could be fatal.
The burden of the disease on the national as well as continental economy is heavy. Malaria costs Africa US$2 billion annually and a poor family living in malaria affected areas may spend up to 25% or more of its annual income on prevention and treatment (10). Malaria remains a major public health challenge for Nigeria, as its prevalence increased from 1116982 in 1990 to 1875380 in 1998 (Federal Office of Statistics). These galloping infection rates with malaria have been made worse by the appearance of strains of the infection which are resistant to cheap chloroquin and thus require more expensive artemisinine containing compounds for their control.
On its part, the World Health Organization (WHO), has also advocated effective low cost strategies for the treatment, control and prevention of malaria. They include the use of insecticide impregnated mosquito nets, the distribution of which is being supported by Shell Petroleum Development Company (SPDC) and the Department for International Development (DFID) in Nigeria. However, improvement of the unhygienic and filthy environment which supports the breeding of the mosquitoes, that are the vectors for the parasites, will remain an important approach in the control of the disease (Fig. 4).
As for diarrhoeal diseases, their significance stems from the dehydration as well as electrolyte and fluid loss which they cause in affected children. Happily, these effects can be prevented or corrected through the prompt use of salt and sugar solution, known as Oral Rehydration Therapy (ORT), prepared and administered at home once the illness starts. The massive health education by which ORT was introduced has paid off as mortality from acute watery diarrhoea has drastically reduced even though the incidence of the disease has not altered to any appreciable extent, indicating that the unhygienic surroundings that give rise to the infection are still with us. This is clearly illustrated in a study that was undertaken at the University of Port Harcourt Teaching Hospital where it was found that with the use of ORT for the management of cases of acute diarrhoeal diseases in children over a seven year period, mortality fell drastically even though the incidence of the disease increased (Fig.5).
Other Considerations
While it is not being suggested that the childhood care that has been put forward impacts directly on the improvement of maternal health which constitutes the topic of our discussion today, there can be no denying the fact that they contribute substantially to ensuring that the mother-to-be grows up in a healthy manner and is in the best possible condition of health at the time she embarks on the key biological process of childbearing. In addition to what has been advanced, the new born female child should be shown love and affection. Nothing should be done to demonstrate a preference for the male child over her. She should not suffer infanticide on account of her sex and she should not have her genitalia mutilated in order to curb her appetite for sexual intercourse at a later age.
The Adolescent Period
Shortly after childhood, the adolescent period begins which is not only a period of phenomenal physical and emotional changes in the young girl, it is also a period when she grapples with peer pressure and may experiment with various issues including sexual intercourse. This period therefore throws up a number of other challenges, a few social, which call for some reflection as they bear significantly on the health of the mother-to-be. They include the vital issues of Female Education, HIV/AIDS and the avoidance of unwanted as well as teenage pregnancies.
Female Education
The importance of education as a tool for social emancipation and for determining the quality of life of an individual and indeed of a nation, is underscored by the fact that it is an important component of Human Development Index (HDI) which defines human wellbeing in various countries. Nigeria’s HDI in 2003 was 0.453 making her a country with low human development.
Furthermore, education is an important determinant of health seeking behaviour of individuals including pregnant women as pregnancy outcome between educated and non-educated mothers is starkly incomparable. By educating the female child therefore, society is directly investing not just in the health of one its mothers-to-be, and the outcome of her pregnancies but also in her ability to bring up her offspring to become responsible members of the community, among many other benefits. Unfortunately, while the majority of Nigerian women have had some form of education, 42% have never attended school. This is about twice the proportion of men who have never attended school (22%) (11).
HIV/AIDS
What makes HIV/AIDS in the mother-to-be a particularly dreadful condition is the fact that she can unwittingly act as a conduit for transmitting the deadly virus to her unborn child through Vertical or Mother-to-Child transmission. This can occur in utero (<10%), during delivery through the vaginal canal (60-70%) and through breast feeding (20-30%) (12). Without preventive interventions, about 25-40% of infants born to HIV positive mothers will contract the virus (6). In mounting prevention and active therapeutic measures in this category of women therefore, the anticipated gain is not only on the mother-to-be, but also, to reduce to the barest minimum the incidence of paediatric HIV/AIDS.
Avoidance of Unwanted and Teenage Pregnancies.
The use of contraception outside wedlock as a means of avoiding unwanted pregnancies remains controversial. But one recognizes the disastrous consequences of induced abortions which follow many cases of unwanted pregnancies especially in single mothers. While more will be said about procured abortion in the section on maternal mortality, the paper advocates for the teaching of Family Health to young adolescents so as to enable them understand their body and how it functions. Such education should contain information on how subsequent fertility and also fetal implantation could be compromised by induced abortions resulting in severe ill health or even death during pregnancy.
Regarding teenage pregnancies, as we all know, there are strong proponents and opponents for early marriage which quite often, is the precursor of teenage pregnancies. But even if early marriage could be defended as a cultural practice, the dangers that are inherent in commencing child bearing as a teenager must be appreciated. Available evidence indicates that many girls below the age of 18 years in developing countries are physically immature to cope with pregnancy and its demands even though their endocrine systems have matured to the point of bringing about a conception. Some of the worst outcomes of pregnancies and child births with regards to maternal and child mortalities as well as the occurrence of serious birth injuries like fistulae have been recorded in this group of mothers (13). One important way of shielding the adolescent girl from the damage that could be caused by teenage pregnancy, is through female education which should engage her and hopefully put her out of reach for marital considerations.
In closing this section of today’s lecture, the point must be made once again that in approaching the process of childbearing, a woman stands the best chance of going through it without problems if she does so in an excellent state of health. The reproductive health issues that have been described for the female child and adolescent, while not directly improving maternal health, help to ensure the wellbeing of the mother-to- be and by extension, improving her chances of remaining healthy as a mother.
Maternal Health
Some of you here received a communication from Dr. Richard Horton, the Editor of the Lancet, requesting you to participate in a series of Questionnaires on three health themes: Child Health, Maternal Health and Community and Developmental Health. The purpose of the communication is to find out from experts like you who are in active practice, what it is that needs to be done in order to improve the indices in the three areas of health care. The exercise is being carried out as a prelude to the creation of well-structured and organized prospective research projects that will form the bases for a global solicitation of support for improvement in these areas of care. We wish to thank Dr. Horton and the Lancet organization for the inclusion of Maternal Health in this very promising work which will direct global attention to the crisis of maternal deaths as had probably not been the case hitherto. For, on the final analysis, poor maternal health and its associated deaths, is our problem, a problem of the developing world.
But SOGON should also take credit for having contributed substantially to beaming the searchlight on women’s poor health in pregnancy and the problem of maternal deaths. Only recently, in July 2004, SOGON submitted a Proposal to the National Assembly in Nigeria for the establishment of an all- encompassing National Institute of Reproductive Health. Unfortunately, the Bill to support the establishment of the Institute did not go through. Furthermore, it was a member of SOGON, Professor Kelsey Harrison, who, in 1985, stirred the conscience of the world through the publication of the findings of the work he and his colleagues did on 22774 consecutive births in Zaria, Nigeria, as a supplement edition of the British Journal of Obstetrics and Gynaecology (14). That publication provided all the hard scientific data that were required to convince everyone that poor maternal health and maternal mortalities in developing countries were tragedies which the international community had neglected for too long. As expected the publication sparked off a flurry of activities in the circle of various governments and development institutions which culminated in the Safe Motherhood Initiatives/Movements that were instituted by many organizations, including the WHO, following its initial conference on the matter at Nairobi, Kenya, in 1987. It is still the realization of the extent of the tragedy that has warranted the inclusion of the Improvement of Maternal Health with a target for the reduction by three quarters, the global maternal mortality ratio by the year 2015, in the Millennium Development Goals of the United Nations. However, this target may be difficult to meet given the fact that estimates of maternal mortality ratios may be as high as 1000 per 100,000 births in some parts of Nigeria (15) and that in these parts, health and other social infrastructures are weak and access to skilled care during pregnancy, labour and the puerperium, limited (16).
Universal antenatal care, supervision of labour by trained birth attendants, the provision of emergency obstetric care when required, as well as skilled puerperal care, which includes care of the new born baby and breast feeding, are essential in promoting better maternal health in developing countries.
Antenatal Care
For antenatal care to be effective in promoting maternal health on a large scale, it has to be universal and domiciled at all three tiers of health care but especially within the ambit of the basic health care that is provided at the Primary Health Care (PHC) level, within the local community where the people live and work. Such care should be provided by the Midwife and not necessarily by the doctor, let alone by the obstetrician and must be backed up by a proper referral system. At screening, pregnancy complications, risk factors for mortality and morbidity, as well those socio-economic issues that enhance ill health and death of the pregnant woman should be identified. What is required next is the basic care of checking for anaemia, oedema and hypertension. Symphysio-fundal height measurements, fetal number and presentation as well as heart tones and the presence or absence of proteinuria, are also confirmed. Where facilities are available, the haemoglobin, blood group and genotype should be known and if possible other laboratory investigations carried out. Referrals to more competent centres should be done at this stage if indicated. It should be the aim of the antenatal care to keep the pregnant woman healthy and to prevent anaemia, malaria and undue rise in blood pressure at all times. Subsequently the routine care should be maintained at designated intervals until delivery or a need to intervene becomes apparent.
Antenatal care should also be used to promote the tenets of PHC by instituting lessons on health education involving topics on basic hygiene, diet in pregnancy, care of the newborn and common complications of pregnancy, among many others.
Arguments as to whether or not antenatal services are critical to the improvement of maternal health or if they ultimately reduce mortality and morbidity are not applicable to Nigeria where the socio-economic environment is harsh and access to health facilities difficult even in cases of obstetric emergencies. Quite on the contrary, maternity care in resource-poor settings as in Nigeria not only enhances maternal health but has also been shown to serve as a potent tool for upsetting some of the harmful effects of large-scale poverty, ignorance and lack of development (16).
Maternal Mortality
The 1999 Maternal Mortality Rates of various zones in Nigeria which were made available by the Federal Office of Statistics in 2003, tell the harrowing story of this unfortunate condition in the country. Far too many women die in child bearing; with Maternal Mortality Rates of 1549 in some parts of the country, Nigeria must be among the countries of the world where the chances of dying as a result of child bearing is highest. Even at that, these deaths are underreported as there is no compulsory registration of births and deaths and no information was provided on two zones of the country, those of the South/South and North Central. Furthermore, the distribution of deaths was very uneven among the zones that were covered by the report; whereas the South/West and South/East zones had rates of 165 and 286 respectively, those of North/East and North/West had rates of 1025 and 1549 respectively. Additionally, far more deaths occurred in the rural than in the urban areas of the country (Fig. 6).
Most of the information one needs in order to appreciate some of the factors that underpin maternal deaths in Nigeria are contained in this brief report. Maternal mortality is least in South/West Nigeria where literacy rates are highest and health facilities more than there are in any other part of the country. In addition, they are better organized than is the case in other parts. Nigeria’s rural communities, where infrastructures are poor, health facilities inadequate and badly run and literacy rates low, constitute the home for the majority of the deaths. Those who died probably did not have access to skilled medical care in pregnancy or in labour on account of social incapacitation or the various forms of delay or they were only able to do so when life threatening complications had arisen in pregnancy, labour or puerperium.
As for the major direct causes of death, most of us here can recite them just as an ardent believer would his rosary beads: severe pre-eclampsia and eclampsia; obstetric haemorrhage; obstructed labour and its consequencies; complications of induced arbortions; genital tract infections (Fig. 7).
SOGON’s findings when it investigated the “Status of Emergency Obstetric Services in Six States of Nigeria” in 2004 were similar to the report from the Federal Office of Statistics: high maternal deaths from all the states that were covered by the study, caused by various forms of delays.
Complications of induced abortions constitute a special problem in Nigeria as it is estimated that as much as 13% of maternal deaths come from this source. Unfortunately, they are seriously underreported and so may not feature correctly in reports that are essentially hospital-based as affected individuals are not commonly brought to the big hospitals. SOGON has sought, so far unsuccessfully, for abortion services to be legally provided on demand in the country.
Credit must at this point be given to the International Project Assistance Service (IPAS) which is represented at this international conference by Mary Luke, the organization’s Vice President, for the introduction of Manual Vacuum Aspiration ( MVA) to Nigeria, through which it has been possible to carry out a speedy evacuation of the uterus in cases of abortions. This expert post abortal care has meant that products of conception are not left to linger in the uterus where they cause haemorrhage and infection that give rise to the often fatal gram-negative septicaemia or the tubal blockage that results subsequently in infertility.
Some of the other direct causes of death as we can see are preventable or can be easily handled if basic maternity care were close to the people and the people empowered and encouraged to use them. In the 2003 Federal Office of Statistics Report to which reference has been made, almost half of the women that were surveyed cited at least one problem in accessing the health care system. The most commonly cited problems were getting money for the payment of treatment (30%) and having to take transport to health facilities (24%). Getting money for treatment was the problem most commonly reported by women of all social groups (11,17). SOGON also corroborated this finding in its own investigation.
Regarding the issue of the availability of skilled care in labour, it is estimated that only about 58% of women in developing countries give birth with the assistance of a trained midwife, doctor or skilled attendance. It is this observation that has encouraged some development institutions to support the training of Traditional Birth Attendants (TBAs) and the use of non-physicians for surgical interventions when serious complications arise during child bearing. These are actions that have received varied responses and under ideal situations should not be encouraged. The answer lies in training and appropriately remunerating health personnel, especially nurses and midwifes, in sufficient numbers that they would be available to undertake their professional responsibilities even in the remote parts of the world.
Maternal Survival Strategies
With regards to what needs to be done in order to bring down the colossal MMRs in many developing countries, including Nigeria, the global obstetric community of which SOGON is part, must now act to produce a set of Maternal Survival Strategies (MSS) similar to what our colleagues in Paediatrics have been able to do under the canopy of the Child Survival Strategies. The paediatricians have identified Growth Monitoring to ensure appropriate overall development of the child, Oral Rehydration Therapy (ORT) to combat fluid and electrolyte loss in diarrhoeal diseases, Breastfeeding as the gold standard of neonatal nutrition, and Immunization to prevent deaths and morbidities from the VPDs, as some fundamental strategies by which the wellbeing of every child can be assured. With these simple measures most of which can be carried out in the homes of parents, the paediatricians are succeeding in bringing down global childhood morbidities and mortalities even though major challenges still remain.
We in Obstetrics should do the same as we already have a number of vital information on the matter. For instance, we now know that growth spurts occur in young primigravidae leading to increased pelvic capacity and that these growth spurts are enhanced by the administration of folic acid tablets to the young girls (14). Knowing the role played by contracted pelvis in the pathogenesis of cephalo-pelvic disproportion and subsequent obstructed labour with the possibility of vesico vaginal fistula (vvf) formation, could it be that the administration of the very inexpensive folic acid tablets to young adolescent girls could serve as prevention for vvf? Also, some of you here participated in the recently concluded Magpie Magnesium Sulphate Trial for the treatment of cases of severe pre-eclampsia. Magnesium sulphate is cheap and if it can prevent severe pre-eclampsia from progressing on to eclampsia and also reduce the occurrence or number of fits in eclamptics, elements which are strong prognostic determinants, why cant we work out a safety regime so that magnesium sulphate can be administered as a first line drug at PHC centres to mothers with severe pre-eclampsia. Furthermore, we know that rapid whole blood transfusion that is required to save lives in cases of massive haemorrhage from placenta praevia, abruptio placenta or post partum uterine atony, is unsuitable for cases of severe anaemia arising from nutritional factors, like iron deficiency anaemias. What is needed in such instances is a slow transfusion with packed red blood cells with the simultaneous administration of a rapidly acting diuretic in order to prevent circulatory overload. We all are also aware that pregnant women who live in holo-endemic areas for malaria infection, and who may have acquired active immunity for the disease prenatally, need protection once they become pregnant to prevent the dangers of malaria in pregnancy, especially in primigravidae. Vaccinations with rubella before pregnancy and tetanus toxoid during pregnancy are also measures whose beneficial effects are well acknowledged by us as obstetricians. Furthermore, the effective use of contraception or shall we say birth control measures saves lives as it cuts downs the number of deaths and morbidities from induced abortions, high parity and conceptions that are too close together. In labour we are conversant with the tremendous contribution that the use of the partogram has made to the prevention of prolonged labour with all its damaging consequences especially in remote communities (Table 1).
There are many more examples that come to mind, specific interventions or treatments that could be targeted at one or more of the major obstetric causes of death. What needs to be done is for us to weave all these together, test their efficacy through operational research and then construct the template of well-structured strategies that can be universally and easily applied and would prevent mothers from dying as well as ensuring their wellbeing.
We should begin to de-emphasise and pull away from the age-long division of maternal deaths along the lines of booked and unbooked mothers. The idea has now served its purpose and has probably taught us all that we need to know: it is the mothers that arrive in hospitals as unbooked emergencies that stand the greatest chance of dying when complications occur in pregnancy or in labour (14). Moreover, the classification is imposing a laisser-faire attitude on us as obstetricians with respect to the unbooked mothers as we are tending to absolve ourselves from any role in their unfortunate plight.
If antenatal care (ANC) is what is required to save lives, then it is our business to ensure that functional ANC backed by a robust referral system is available to all women irrespective of where they are. We must work out a system whereby the supervision of pregnancies and the deliveries of all uncomplicated cases at the first level of care would be skilfully handled and a functional referral system which would direct those with complications to well-equipped centres where appropriate expertise, especially those for carrying out operative interventions including the administration of anaesthetics and blood transfusion, exit, for further management. And of course such centres must have the most basic requirements of clean water and electricity supply.
The path to achieving MDG5, a comprehensive package of care commencing from the early childhood of the female child, through to the adolescent period and extending to pregnancy, as is indicated in fig. 8, is self-explanatory. The MSS constitute a summation of the components of this pathway with selected interventions that should be targeted at specific major causes of maternal deaths.
Happily, SOGON has already made a start through its previous studies and actions. At this year’s International Conference, the society is also going to “unveil a presidential bull by the horn approach to drastically reduce our maternal mortality ratio.” In this respect, I wish to suggest that SOGON takes the lead and carries this strong position to the various development institutions that have interest on the issue of maternal health, especially FIGO, as the society now has a formidable representation in that body, in the person of Professor Friday Okonofua, our immediate past Secretary-General.
The Current Situation
Since Nigeria obtained independence from British colonial rule in 1960, the pangs of national development have been severe and excruciating. Lurking from one military rule to the other in a higgledy-piggledy manner, the national polity had been characterised by instability. Failed economic and agricultural policies, like the Structural Adjustment Programme (SAP) and Operation Feed the Nation (OFN), as well as government’s inability and unwillingness to address crucial state issues have resulted in considerable decline in the economy especially since the 1980s. This decline has eroded the purchasing power of the national currency, deepening poverty and fuelling incessant communal unrest. The harsh social environment stalled development, exposing the most vulnerable, women and children, to some of the ravages and stark realities of underdevelopment: poor nutrition, frequent ill health, and high mortality rates, among others.
Dithering then, as it were, on the precipice of a failed state, Nigeria elected a democratic government in 1999 led by Chief Olusegun Obasanjo. That government, which has now been in place for over seven years, the longest since independence, has succeeded somewhat in pulling the country from the brink. Although political stability has not been completely restored, instability such as there is, has taken place within the compass of democratic governance buttressed by the rule of law. As one of the founding fathers of the new vision for the renaissance of the African continent, through the New Partnership for African Development, (NEPAD), the government has fought corruption on an unprecedented scale and has embarked on far-reaching reforms which are aimed at good and accountable governance and a redirection of the nation’s socio-economic path. It launched the National Economic Empowerment and Development Strategy (NEEDS), a comprehensive socio-economic reform package that incorporates the MDGs, and one within which greater transparency has been introduced into the conduct of government business through Due Process. In addition, the government has pursued an aggressive policy of demanding and receiving debt reprieve, the proceeds of which it has ploughed back into MDG specific spending. With the growing commitment of state as well local governments to poverty reduction, through the State Economic Empowerment and Development Strategies (SEEDS) and the Local Government Economic Empowerment and Development Strategies (LEEDS) there is a possibility that some of the MDGs will be achieved.
As a result of the improved management of the economy, the growth rate of the GDP averaged 8.2% between 2002 and 2004 against the average annual growth rate of 3.5% in the last decade. For the first time in a decade therefore, the growth rate of the GDP has exceeded the growth rate in the population and the nation’s foreign reserve, a measurement of the economic performance of the country, now stands at 45 billion US dollars (18), although many have argued that this increase in the nation’s wealth has not been seen to improve the living conditions of its citizens.
The world has made significant progress in achieving some of the MDGs. Between 1990 and 2002 average overall incomes increased by approximately 21%. The number of people in extreme poverty declined by an estimated 130 million. Child mortality rates fell from 103 births per 1000 births a year to 88. Life expectancy rose from 63 years to almost 65years (7).
Furthermore, the World Bank recently pointed out that countries like Ghana, Burkina Faso, Cameroon, Mozambique and Uganda have taken concrete steps which have lifted significant percentages of their citizens out of the poverty level. Although Nigeria was not included on the list, the current situation with respect to the economy gives one some optimism with regards to the issue of poverty alleviation in the country and ipso facto, to some mitigation of the disastrous consequences of extreme poverty on maternal health (19).
Conclusion
The will that has been demonstrated by the international community to achieve the MDGS, including MDG5 is laudable. It has led to the invigoration of existing development agencies and the establishment of new ones. The Global fund for the Eradication of Malaria, Tuberculosis and HIV/AIDS is a good example. While in Africa, where some of the poorest countries in the world, with little or no development, exist, there is now NEPAD. For in the final analysis, poverty is it and “poverty is a reality” as Mr. President himself said only last friday at the 58th Foundation Day Ceremony of the University of Ibadan (20). Poverty is at the heart of the matter regarding the difficulty Nigeria as well as many other sub-Saharan African countries are facing in meeting the MDGS and to alleviate poverty, Nigeria must increase the opportunities for economic advancement while concurrently providing essential social services to the poor.
Bangladesh with a population of 150 million, with frequent natural disasters and catastrophic seasonal floods, has now banished famine and put poverty on the retreat through a well-organised social empowerment scheme for the very poor, most of whom are women, through the Grameen Bank which was established by Mohammad Yunus, a university professor of economics and the recipient of the 2006 Nobel Peace prize. With an HDI of 0.345 in 1975 Bangladesh belonged to the group of low human development countries. By 2003 its HDI had moved up to 0.520 with the country placing among medium development countries.
Improving Maternal Health remains an important component of the MDGs and SOGON, in addition to all that it has done so far, must now take definite steps to bring down the maternal mortality ratio in Nigeria, which is at the core of the improvement of maternal health. SOGON should insist on the compulsory registration of ALL Births and Deaths as well as the collection of vital data in the country. In addition it must put in place well-structured Maternal Survival Strategies by which basic maternity care with targeted interventions, within the umbrella of PHC, backed up by a well-organized referral system, is brought to the door step of every woman in Nigeria, irrespective of where she lives.
As for the 189 nations of the world that met in September 2000 to articulate the eight MDGs, one must say bravo, because if properly executed, the MDGs hold the key for the release of the wretched of the earth from the shackles of the dehumanization of abject poverty. For as was said by a celebrated Roman poet, In great human endeavours even to have had the will is enough.
Just two weeks ago, I was walking on Gerrald Street West in Toronto, Canada, from my room at the Delta Chelsea Hotel to the University of Toronto, where I was scheduled to hold a meeting with the authorities of the university. In risking the walk on that nippy early November morning despite the drizzle, I was testing out, as it were, the extent of my recovery from a common cold that had taken hold of me following a protracted wait at various airports on account of flight delays and cancellations on my way to Canada.
As I walked close to the Toronto General Hospital, I came across a huge billboard on which was inscribed
“INVESTMENT IN CHILDREN PAYS BIG DIVIDENDS”.
The statement had been placed on the billboard by the Ontario English Catholic Association and so bold were the letters that it was intended that even the blind should read it. I decided to ignore it not being a paediatrician but so strong, arresting and impactful was the message, in contrast to its scantiness of words, that I really could not do so. And so, I stopped, copied it and decided that I was going to end my address today to this august body, with an edited version of that communication in this age of laptops and computers. The message is for us, members of this great society, the Federal Government of Nigeria, the 36 state governments, the 774 local governments, as well as the various development institutions that are operating in the country and indeed for all Nigerians. And the message is:
“INVESTMENT IN MATERNAL HEALTH PAYS BIG DIVIDENDS”.
Acknowledgement
I wish to thank Professor Raphael Oruamabo and Dr. Samuel Uzoikwe, Director of the Institute of Maternal and Child Health and Senior Lecturer in Obstetrics and Gynaecology respectively at the University of Port Harcourt, Nigeria, for allowing me the use of their slides. Professor Oruamabo also read through the script and made useful suggestions. I am indebted to Mr. Biodun Elias, my personal assistant at the National Hospital, Abuja, Nigeria, for secretarial help.
REFERENCES
13. Briggs, N.D. (1989) ‘Outcome of labour in occipito posterior
positions in an African population’, British Journal of Obstetrics
and Gynaecology, 10, 1234-1236.
14. Harrison, Kelsey A. Child Bearing, Health and Social Priorities:
A Survey of 22774 Consecutive Hospital Births in Zaria, Northern
Nigeria. Br. J. Obstet. Gynaecol. Supplement Number 5, October
1985.
15. Uzoigwe, SA; John, CT. 2000. A ten year review of Mateernal
Mortalitiy at Port Harcourt Nigeria. Nig. J Clin Pract. Vol 3 (21),
80-84.
16. Maternity Care in Developing Countries. Eds. Lawson,
JB; Harrison, KA; and Bergsrom, S. RCOG Press Publishers.
17. Nigeria. Millennium Development Goals. 2005 Report.
18. Independent Day Broadcast, 1 October, 2006. Chief
Olusegun Obasanjo, President of the Federal Republic of
Nigeria.
19. World Bank African Development Indicators Report 2006
20. “Poverty is a reality”. Chief Olusegun Obasanjo, President and
Commander-in-Chief of the Armed Forces of Nigeria at the 58th
Foundation Day Ceremony of the University of Ibadan, Ibadan,
Nigeria, Friday, 17 November, 2006.
Figure 1
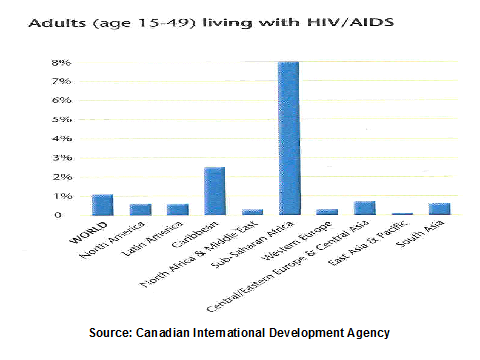
Figure 2
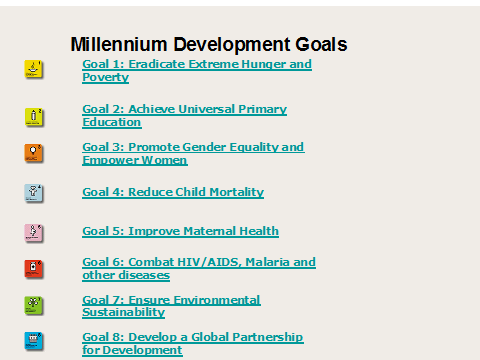
Figure 3
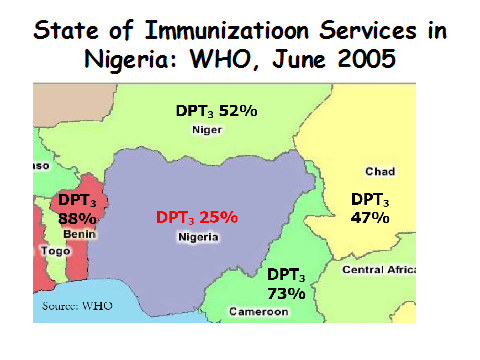
Figure 4

Figure 5
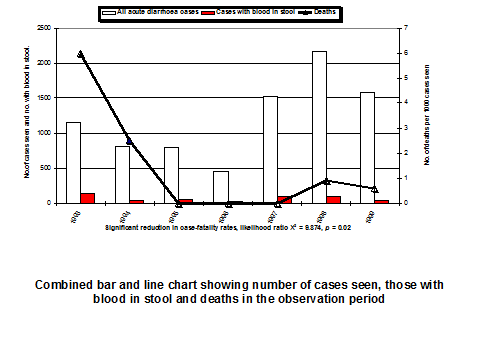
Figure 6
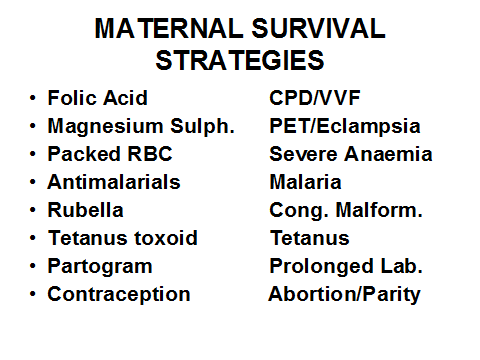
Table 1
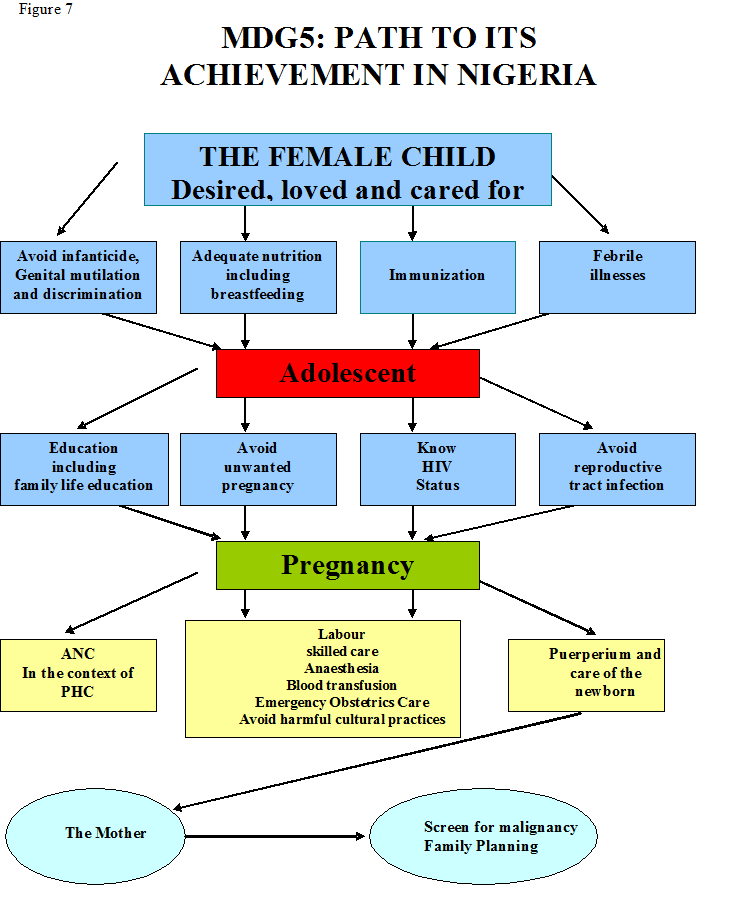
Figure 8
MDG5: What Path leads to its Achievement in Nigeria? A Guest Lecture by Nimi D. Briggs. On the occasion of the 7th International Conference of the Society of Gynaecology and Obstetrics of Nigeria (SOGON) on Wednesday 22 November, 2006
Former Pro-Chancellor and Chairman of Council, Federal University, Lokoja, Nigeria. February 2016.
Member, Court of Governors, College of Medicine, University of Lagos, October 2015 for four years.
Copyright © 2025 Prof Nimi Briggs. All rights reserved. Designed by Syllable Media Limited +447869717613